
display screens for memory impared manufacturer

This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data.

A screen magnification system enlarges text and graphics on a computer screen. It is loaded into the computer’s memory and functions similarly to a magnifying glass moving over a page, following the cursor, and magnifying the area around it. Using a mouse or keyboard commands, a user positions the cursor on the section of the screen to be magnified or has the cursor move automatically across and down a magnified page at a preset speed. The magnified area may also be emphasized with color and shading, so that users who lose their place on screen may easily locate a magnified area. Fonts used in magnification programs are usually designed to smooth out the jagged or “stair-step” appearance of computer-produced diagonal or curved lines. Today’s full-featured screen magnifiers can magnify all items on a screen, including the mouse pointer, text cursor, icons, buttons, and title bars. The magnifiers also provide a set of mouse tracking features.
Persons with considerable vision may not need a screen magnification program. Instead, they may use a larger monitor that allows for larger text or graphics while keeping all material on the screen. Larger text and graphics can be achieved by lowering the screen resolution so that bigger pixels are used.
In addition, the appearance of objects or texts on a screen may be altered using the accessibility wizard in a Windows system, which provides a number of options. These options include adjustments for the font size, screen resolution, scroll bar size, icon size, color scheme, mouse cursor appearance, and mouse cursor blink rate. The main accessibility feature in Windows, however, is its screen magnifier which can also be set up through the accessibility wizard. Although the default color scheme in Windows is black text on a gray background, this can be changed to be more easily distinguished using one of Windows high-contrast color schemes.
Portable battery-operated and braille-compatible screen reader and scanner with a built-in screen for displaying photos, magnifying small objects and enlarging texts for individuals who have difficulty reading printed text.
Lightweight, battery-operated, portable scanner and reader that comes with a pair of headphones that easily plugs into the front of the device for privacy. The ergonomic thumbwheels and tactile controls are intuitively located for ease of use. Braille-display compatible for reading a book or a menu at a restaurant or filling out a form at the doctor"s office. Incorporates the AudioMinder technology, allowing the user to set an alarm and record appointment reminders.
Fast, accurate, and easy-to-use scanning and reading appliance that connects to a monitor or TV to display text in a high-contrast, large font so user can read along as the content is spoken. May be used for scanning a printed page, pill bottle, recipe card, or newspaper. Motion detector automatically senses when a new page is placed under the camera.
Screen magnification and screen reading software for Mac users. Provides magnification, contour enhancement and pointer settings as well as screen reading with high-quality speech output. In addition to text to speech voices, such as Infovox iVox by Acapela, it comes with automatic language identification in the screen reader mode and GhostReader, an application for reading documents. GhostReader contains shortkeys for fast and easy access to the text and the user can listen to documents including file types such as Text, Word, HTML, PDF, ODT or RTF. Also allows user to save texts as Mp3-files to be played in iTunes, be uploaded to an iPod, iPad or burned onto a CD.
Compact and portable lightweight reading device that scans and reads text documents such as books, newspapers or bills with a push of a button. May be connected to an external monitor via VGA and HDMI connectors and has 8 zoom settings. Offers fully readable letter size with an option for column recognition and allows documents to be stored for later use. Has a standard audio jack for headphones or external speakers. Internal battery available for portability.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices. Allows users to write map files to make nonstandard applications usable.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices.
The sense of smell is one of the most powerful ways to trigger memory activation via sensory stimulation. There are also therapeutic benefits, specifically with regard to some of the behavioral symptoms associated with Alzheimer’s and other forms of dementia, that aroma-based stimulation can achieve. We have designed our Memory Lane TV solution from its inception to be multi-sensory, to maximize the benefits achieved from stimulation of as many senses as possible in a coordinated, harmonized way.
We have paired much of the content with proven aroma scents to enhance the experience and therapeutic benefits for the person living with dementia. Most people will experience even greater benefit with regard to managing behavioral symptoms when leveraging the reinforcing power of harmonized multi-sensory stimulation.

The Digital Exam Enables Providers, For The First Time Ever, To Quickly Screen Brain Health During A Typical 40-Minute Wellness Appointment, More Efficiently And Accurately Signaling Early Signs Of Cognitive Decline
(PRESS RELEASE) Neurotrack, the leader in science-backed cognitive health solutions, announced today the launch of the first ever three-minute digital cognitive assessment that enables providers to quickly screen for cognitive decline and impairment which can be an early indicator of neurodegenerative diseases such as Alzheimer’s during their annual wellness exam. This solution could increase the number of annual cognitive assessments completed and provide additional opportunities for early intervention.
In a sample survey of adults with either Medicare Advantage (MA) or fee-for service Medicare, only about a quarter of those enrolled say they received an evaluation (link to citation), despite CMS guidelines that require cognitive assessments as part of annual wellness visits for Medicare beneficiaries enrolled in Part B.
Neurotrack’s digital exam has been designed to fit easily within a typical primary care annual wellness visit or alternately empower patients to independently assess their cognitive health and share the results with their providers. The easy-to-use assessment can identify patients with cognitive impairment in just three minutes, with better accuracy compared to traditional methods and uses culturally-agnostic symbols and numbers to reduce bias in testing for those with other languages, backgrounds, and cultures. For providers, it offers a scalable way to screen patients for potential cognitive issues, regardless of symptoms.
“Early detection is critical for patients facing a diagnosis like Alzheimer’s or dementia, but unfortunately most patients aren’t screened for cognitive impairment until they show symptoms, which can appear more than 20 years after initial brain changes have occurred,” said Elli Kaplan, founder and CEO of Neurotrack. “We want to empower providers to integrate cognitive testing as a new vital sign in annual physical exams starting at age 65, with the hope that an earlier diagnosis for patients with dementia will lead to more effective interventions.”
There are a number of converging factors driving the need for cognitive screening at scale, including an aging population and a critical shortage of neurologists, neuropsychologists and providers specializing in senior care. With a projected one in 10 older adults expected to develop Alzheimer’s, the U.S. will need to triple the number ofgeriatriciansalone by 2050 in order to care for them.
“The need for this type of diagnostic tool, at this time, cannot be overstated,” said Dr. Jonathan Artz, a neurologist at Renown Health, who is a Core Member of a Statewide Planning Team to develop a Nevada Memory Care Network that would include a cognitive health screening platform. “Neurotrack’s technology would make cognitive assessments as part of the yearly Medicare Wellness Visit more manageable and efficient for primary care providers. The Neurotrack offering is well designed and has the features necessary for integration into the Nevada Memory Care Network.”
Dr. Artz added, “Neurotrack’s solution is grounded in proven methodologies that are scientifically validated and can detect possible cognitive impairment. Using this tool within a clinical workflow opens up the possibility for every senior to be screened in a more timely manner and earlier, when an intervention can be most effective.”
“With a rapidly growing aging population and new factors stemming from COVID and the social isolation many experienced during the pandemic, cognitive decline is a significant concern for people over the age of 65. There’s a critical need for these kinds of assessments,” said Dr. Andrew Cunningham, a practicing physician who also serves as a clinical services director for Neurotrack. “This screening tool was designed by primary care physicians for primary care physicians to meet this need and empower providers to better care for their patients.”
Neurotrack is currently developing a new “digital therapeutic” to delay or prevent cognitive decline when early signs are detected. As part of this work, the company is conducting a clinical study in collaboration with researchers at the University of Arkansas to look at the effects of health education and health coaching on cognition and cognitive risk factors, using grant funds from the National Institute on Aging. Preliminary results show significant reduction in symptoms after one year of intervention: thinking and memory improve, and depression and anxiety lessen.
Neurotrack recently secured $10 million in new funding to support and accelerate its successful go-to-market push with leading health systems and providers across the country and to continue the development of a provider-based solution for those identified with cognitive decline. The latest funding is supported by experts in a range of disciplines including technology, clinical care, biotech, patient advocacy and caregiving.
While continuing to expand their clinical interventions and scientific excellence, Neurotrack has engaged physician leaders from family medicine, geriatrics and geriatric psychiatry to form a new clinical advisory board. The board will advise Neurotrack in order to better meet the needs of patients as well as physicians and health systems caring for our aging population.
Neurotrack is a digital health company on a mission to transform the diagnosis and prevention of dementia and Alzheimer’s disease. The company develops clinically validated digital cognitive assessments, using eye-tracking technology, to measure and monitor the state of one’s cognition. The company has also developed a comprehensive cognitive health program that enables individuals to make lifestyle changes to strengthen their cognitive health as they age. Neurotrack has published 22 peer-reviewed papers and its solutions have been recognized by leading organizations including the Cleveland Clinic and the National Institute on Aging. Working with providers, health systems and employer partners, Neurotrack has enabled more than 150,000 cognitive assessments on its platform. The company is based in Redwood City, CA. For more information visit www.neurotrack.com and/or follow Neurotrack on LinkedIn and on Twitter.
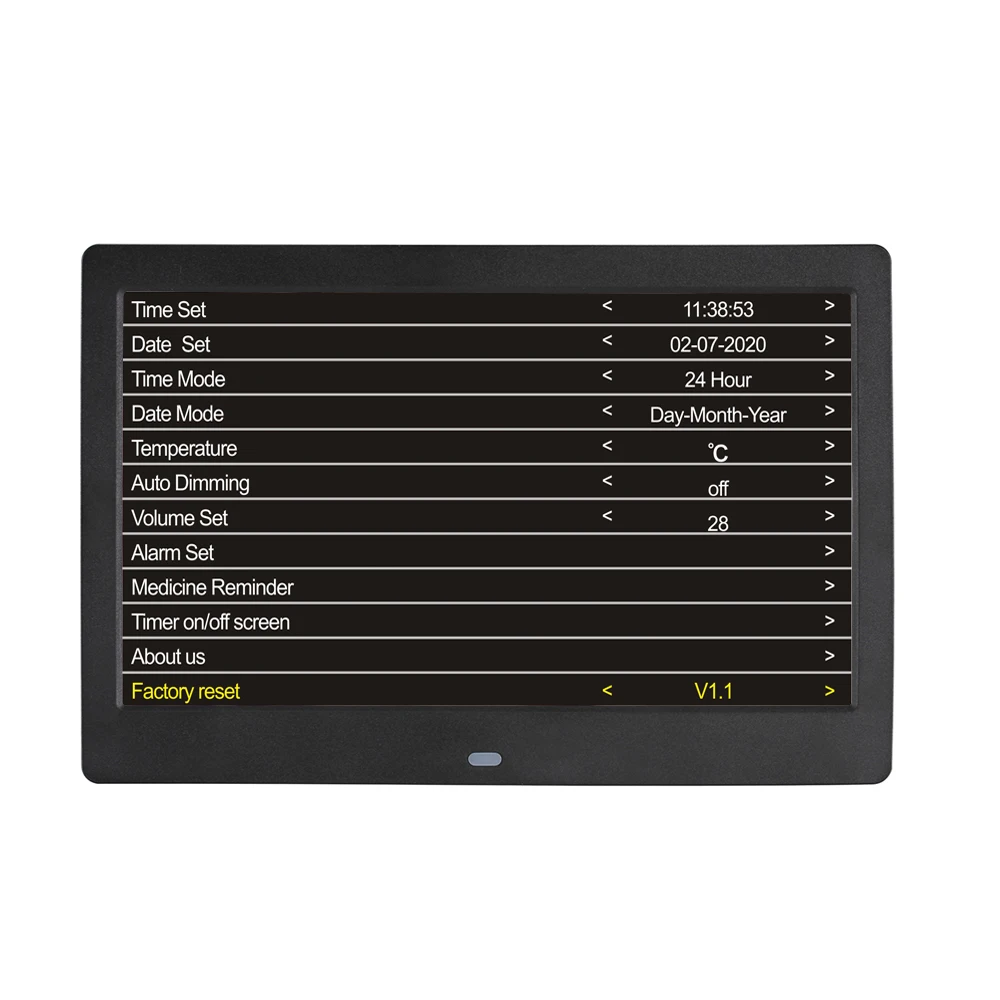
This review is specific to the "SVINZ 3 Alarms Dementia Clock, 2 Auto-Dim Options, Large Display Digital Calendar Day Clock for Vision Impaired, Elderly, Memory Loss, Black, SDC008W".
This device is basically just a regular clock internally, so it is the "form factor" and display that makes the difference. It has the form of a medium sized black picture frame with a "picture" of the day and date and time in large lettering on a pure black background that almost merges with the frame. There is no animation or funny business with the display; it is always there, displaying in very large, clear text, the DAY of the week (no abbreviations, it is completely spelled out), then the part of the day in somewhat smaller, although still large letters, with the possibilities being MORNING, AFTERNOON, EVENING, NIGHT, and PREDAWN. Then, in very large text, is the time of day, e.g. 10:30 A.M.. Then in somewhat smaller text is the completely spelled out month, numeric date, and complete numeric year, e.g. DECEMBER 4, 2019. That"s all there is, and its format does not change. The makers of this product apparently recognize that changing formats, abbreviations, and animations will only be confusing to elderly folks (or anyone else who prefers their information unmolested).
Both of my folks" clocks powered up from the factory with the correct time and date information already set; only the hour display was off by two hours.....I suppose the clock was set for one time zone while they are in another time zone.
The clock has some sort of internal battery, or equivalent non-volatile circuit that allows the time to be kept even during times when the clock is not powered, either when not in use or during power outages. But the display DOES NOT appear until the clock"s included AC power supply is plugged into a wall outlet. Note that the power supply has a DC output, which means that the clock cannot synchronize itself with the AC power line frequency, which is something that many (most?) digital clocks do. And as far as I can tell, this clock is not synchronized by radio waves from the US Atomic Clock, nor do I believe that it is synchronizing to the GPS timebase. What this means is that the clock is working internally just like a digital watch, basing its timekeeping accuracy solely on its internal clock crystal. Accordingly, you must expect to make minor time adjustments periodically; hopefully only a few times a year.
Also on the back of the clock is a fairly large set of navigation buttons, nicely marked in high contrast white on the black background, making it very easy to see and use. Pressing the MENU button causes the clock display to be replaced by a clock menu. Then you press the UP and DOWN navigation buttons to scroll vertically through the menu until the desired item is selected (its text changes from white to yellow). Then the LEFT and RIGHT navigation buttons are used to change the current selection, and the OK button accepts and stores your change, and you can navigate to another menu item. When you are done making changes and want to return to clock mode, just press MENU again. This is about as intuitive and easy to remember and use any any system out there.
Some menu items, besides the obvious setting of date and time, include selecting 12 or 24 hour mode, and selecting between white text and yellow text on the clock display, and selecting the "auto dim" feature between OFF, MEDIUM, and HIGH. You can also set up the optional alarms, and there are three possible alarms that can be set. I have not used the alarms and so cannot comment on them.

I can’t thank you enough for working me to get the phone up & running for my mom. She’s starting to adjust to using it. This phone will help her as she gets flustered with all the options even on a basic cell phone.
I am so grateful for this phone & the wonderful support staff that helped me with my questions & missteps. Tried out the phone with family members & are anxious to give it to her on Monday, her 92nd birthday. This will be a godsend for her to be able to communicate with her family during these difficult times. Usually there are only 5 stars but would give 10! Thank you for making this a very bright moment. Thank you again.
I have been looking for a phone that would not confuse my Mother with her dementia. I have not found a phone that would work for her until I found this one. Having the ability to set up and control the phone from the caregiver portal has greatly reduced the time I have to spend dealing with phone issues. My Mother lets me know if she needs to add a number to her list and I can do the from anywhere without having to physically change it on her phone. I also like being able to check the battery level from the portal adn let her know if she needs to charger her phone if she forgets. No more assuming the phone is just dead. The GPS feature also gives me peace of mind to know were she is or if her phone was left somewhere. This is a great solution if you are looking for a phone for your family member with dementia.
I am so very thankful for this phone. It has given my father a sense of freedom again. His confidence in using the phone is phenomenal and we haven’t been able to say that in a while. I am wondering if there is a case that can be recommended that has a cover for the front that will stop accidental calls. PLEASE LOOK AT THIS PHONE FOR YOUR LOVED ONE, YOU WON’T REGRET IT.
I purchased this phone for my mom who has dementia and was having great difficulty using even her simple flip phone. It is very easy to use and wonderful that I can manage the phone from the portal. I would rate “5” except 1) I assume there is no way to disable the 911 function due to legal issues, but it would be nice if I could since she is in a nursing home and help is always nearby; 2) would be nice to get rid of the message that says “individual’s voicemail has not been set up” since there is no voicemail option (I get calls from my mother’s family asking why she has no voicemail); 3) would be nice to be able to increase the number of rings. It only rings four times and it usually takes her longer than that to get across her room to answer since she doesn’t carry the phone around with her. All in all, though, very happy with this purchase.
As for 2) the voicemail message and 2) the number of rings – these are control day the wireless provider. The number of rings / ring duration can bu adjusted by some of the carriers. Please contact the carrier and request it to be changed.
This phone is very nice to look at and easy to use. I love that we can limit the calls that my mom receives. She was always so confused by the spam calls about the extended warranty for her car. It’s great that she doesn’t get those anymore. It’s also really nice that she can see photos of my sisters and me to decide who she wants to call.
However, there are a couple of things I do not like. One, the volume is fixed, and it is too loud for certain situations. Secondly, there is no way to track missed calls, or voice mail.
This phone solved our conundrum with needing a simple phone for our older guy who now feels reconnected without the barrage of incomprehensible scammers. The tech support and customer service is responsive, efficient and superb.
I just wanted to say thank you for this product. My mom, who has dementia, broke her hip, got COVID while in the hospital and ended up recovering from both in isolation in a nursing facility. She has been struggling to understand what is happening to her and not being able to be there with her has been a challenge for all of us. This phone has helped her tremendously. She had forgotten how to use a cell phone a long time ago but she can use this phone and it has lifted her spirits to stay in touch and she likes looking at our pictures. It’s such a well designed product and the customer support you offer is very appreciated as well. The staff at the Verizon store wrote down the information because they said they get requests for senior-friendly phones all the time and they don’t sell anything like this phone. The therapy staff at the nursing home commented that they love the phone as well and will be recommending it to other families in the facility.
This phone has been a godsend to me as the caretaker of my mother from three states away. I love how I can manage the phone via the portal. There are so many things I love about this phone and its ease of use for my mother. Other reviews talked about the default ringtone volume being very loud and unable to change. The ringtone volume was super loud! I called RazMobility Support and they walked me through how to lower the ring volume (but you can only do it when having the phone physically with you and they walk you through all of the steps). I’m sure there are other changes RazMobility support can help you with. Just call them and ask, “Can _____ be adjusted on the phone?” They have been super helpful. I love how simple the portal is to manage and how I can see the battery life, and GPS location of my mother’s phone. The MintMobile cell service did not do too well in my mother’s nursing home, but it was easy to switch out the SIM cards to another carrier. But make sure you purchase the more expensive Raz phone so you can easily switch carriers if you need to. I would have stayed with MintMobile if the reception was better as their website is super easy to navigate. So this review doesn’t go on forever, I’ll focus on some features I would like to see in the future: recent call list, ability to adjust the ringtone volume, voice volume from portal. One glitch I’ve found is that when my mother presses the “Hang Up” button too long, she accidentally calls the contacts listed in the #5 & 6 spots. To avoid her accidentally calling someone a lot, I added my contact info into slots 5 & 6. So if it happens, she is just calling me. We also bought the wireless charger (which comes with the protective phone case). That way my mom does not have to struggle to plug in the regular phone charger. The wireless charger charges super slow to avoid wearing out the battery. This phone is awesome. Raz, if you created an affiliate program, I think you could get the word out even more about this phone. I would be a huge cheerleader of the phone!
I purchased this phone for my Dad who we just moved into a nursing home due to dementia. He became unable to remember how to work his old cell phone or the regular telephone. The RAZ has been a Godsend. It’s so easy for him to use and he is absolutely thrilled to be re-connected with his family. I had a little trouble activating it, ( a senior citizen setting up a phone for a senior citizen…what could go wrong???). But I called customer service and the rep that helped me was amazing. Patient and knowledgable and even emailed me pictures of what things should look like along the way. She made sure I knew how to add names and pictures to the phone and even offered to do it for me if I emailed her the pictures. I’ve called a few times with questions and I reach a human being quickly and they always know the answer to my questions. Customer service of the highest caliber. So far the only downside is that when the phone is in the case the volume of the ringtone is very low and my Dad doesn’t always hear it. I’ve called customer service and they told me that I have to be near the phone to adjust the volume, so the next time I am there I will give them a call. The RAZ is the absolute perfect cell phone for any senior but especially one who has impaired mental capabilities.
My 92 year old father loves this phone. I love not worrying that someone is scamming him over the phone. He loves showing it off to his friends at the retirement community. I love not spending hours trying to talk him through getting him back on his phone. He loves not calling the wrong person because he touched the wrong line in his contacts. I love updating new phone numbers for his contacts without having to have his phone in hand. For us it’s a win/win/win
My Dad doesn’t have dementia but is 87. We got the Raz phone and it’s like a long, cool drink of water. We tried Jitterbug and Jethro “senior friendly” phones and they were a JOKE. Raz is the first truly SIMPLE phone – no menus, God bless them, and remotely configurable. The only thing I would criticize, and I hope Raz is listening… About once or twice a day, the Raz phone makes an outgoing call while in my Dad’s pants pocket. I have witnessed this first-hand. He’s puttering around the kitchen, not bending over, not with his hands in his pocket, and his phone calls me. If he were allowed to “turn off” the screen before he puts the phone in his pocket, I believe the problem would be fixed. We did try a belt holster, but with his posture, his belt is too close to his armpits and it takes so long to get the phone out of the holster that the phone stops ringing before he can answer.
I purchased this phone for my brother who has rapid arm and hand tremors due to Parkinson’s Disease. He also has early Dementia. He is not tech savvy at all. The Raz phone is truly a blessing to him and my family not only because it’s simple and easy to use, but it eliminates the clutter he would have to navigate through using the traditional smart phone. He is proud that he has a device that is fully simplistic and streamlined to his need, but also instills his dignity just by the phone’s impressive appearance. Raz mobility technical support is Fantastic! I have dismissed products from other companies just on the premise of customer support alone, regardless of the quality of product. I was helped by Alex at Raz Tech support. He was extremely knowledgeable, methodical, courteous, and above all, patient. I enjoyed one of the best customer experiences I have had in many months. Kudos to Alex.
I found the RAZ Phone easy to get set up and it works as advertised. This will be a big help as my wife has memory problems. Now I feel comfortable being away from her for a while. Thanks.
Great phone for those with dementia. Easy to set up from the caregiver portal. Customer Service is great. An improvement would have the phone shut off automatically if not being used since the battery goes down and the phone has to be charged daily.
I recently returned my mother’s Memory Cell Phone because someone at her care facility had inadvertently exited the app and did a factory reset. Within a week, I had the phone back with the app reinstalled. Not only that, you installed the new version which has great new options AND sent a complimentary wireless charging platform because she had damaged the charger port trying to put the charger in the wrong way. That is customer service above and beyond.
This is close to being the perfect phone for those with dementia and those of us who care for them. It is so very well thought-out, anticipating all the problems. For the first time in months, my husband can call me when he’s feeling anxious or worried from his memory care facility. It has been such a relief for both of us.
The Memory Phone has been a wonderful solution to our parent’s dementia challenges. What a relief to have the confidence that they can call when they want and not be discouraged by the complexity of a smart phone.
The RAZ is a great phone. Customer service is outstanding. I bought this for my Mom who has Alzheimer’s. Unfortunately we waited a little to long to make the change. She was not able to make the adjustment to the phone and I had to return it. With that being said, this is a wonderful cell phone, I am super impressed with how it works and the options for the caregiver from the portal. I will be telling anyone I know who needs this service. We did the T-Mobile version and had zero problems. Just put the SIM card in and it worked perfectly. Thanks for a great product!
RAZ MEMORY phone is exceptional for my father in law age 94. He has some age related dementia combined with macular degeneration. Especially helpful are the auto answer to speaker phone options. He is able to call us usig the limited photo buttons. And, NO MORE JUNK CALLS. Wish we were aware of this earlier. We are showing it off at his new Assisted Living Community. We also love the optional charging cradle which is home for the phone most of the time.
This phone is fabulous for my mom who has dementia. We tried several ‘easy’ and ‘senior’ phones before finding this one. This is the only one she’s been able to use reliably. Being able to control the phone settings from my phone is great; no more deleted contacts or turning her phone off then wondering why it wasn’t working. The phone works well on the T-Mobile network. I had to contact customer service and was shocked to be connected to a person right away. He immediately identified the issue and walked me though how to fix it. The call lasted maybe 5 minutes and there have been zero issues since. I wish we’d found this phone a couple years ago. It would have saved both mom and family members a lot of frustration.
Easy for my non-tech husband to use. We set it to auto answer and speaker phone, so he doesn’t even need to pick it up. Makes us feel more secure for those times when I need to leave him alone for short periods.

The information on this website is for general informational purposes only. No information contained here should be construed as professional medical advice. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking treatment because of something you have read on this website. References in this website to any third-party products, services, processes, hypertext links to third parties or other information by trade name, trademark, manufacturer, supplier or otherwise does not necessarily constitute or imply its endorsement, sponsorship or recommendation by Soo Borson or the administrator(s) of this website. Links to other websites are provided for your convenience and Soo Borson and the administrator(s) of this website disclaim any responsibility for the content, accuracy of the information and/or quality of products or services provided by or advertised on these third-party websites.

Mutation analysis was carried out using Sanger sequencingPSEN1 or APP were assessed for the presence of additional mutations in other dementia-related genes using the Medical Research Council Dementia Gene Panel
All methods were performed in accordance with the relevant guidelines and regulations. The study was approved by The National Hospital for Neurology and Neurosurgery and Institute of Neurology Joint Research Ethics Committee (subsequently, National Research Ethics Service Committee, London Queen Square, REC ref 11/LO/0753). Written informed consent was obtained from all participants.
The study protocol included the “Object-localisation” VSTM taskhttp://sprott.physics.wisc.edu/fractals.htm). Following Liang and colleagues’ finding that testing confined to only 50 trials was sufficient to distinguish FAD cases from controls2). Periods between saccades were defined as fixations. A 9-point calibration and validation were performed prior to the experiment. All the data were obtained from recordings with an average Cartesian prediction error of < 1° during the validation. A drift correction procedure was used before each individual trial.
In addition to identification accuracy and localisation error, two additional outcome metrics of task performance have been used in previous publicationsS1).
All eye-tracking recordings were visually inspected using Data Viewer to check for any signal loss that would interfere with data analysis and interpretation of results. Blinks were identified and removed using Eyelink’s automated blink detection. Vision was binocular but only eye movements from the right eye were recorded.
In order to test the hypothesis that encoding—indexed indirectly by the overall time spent fixating a stimulus—might be particularly affected in presymptomatic FAD individuals, we examined four metrics related to perception of the stimuli. An assumption that we wanted to check was whether one reason for variable or poor performance was not having spent an equal amount of time processing the details of each fractal. This metric will be referred here as “equality” (see below).
The eye-tracking measures capturing exploration strategies (for each trial) during the 3-s viewing period were:Total dwell time on fractals: sum of the total fixation time on all fractals.
In order to account for any low-level oculomotor differences, we also evaluated basic oculomotor metrics (defined for each trial) between groups using Eyelink’s automated detection algorithm:Saccade amplitude (deg): average amplitude of each saccade.
Baseline demographics and neuropsychology scores were compared between controls and each of SMCs, late PMCs and early PMCs using ANOVA (age; NART; verbal and performance IQ; arithmetic; digit span backwards; verbal and category fluency; GNT; spatial digit span forwards or backwards) or Kruskal–Wallis test where the distribution of the variable was skewed (MMSE; education level-in years; CDR score; anxiety; depression; self-reports of subjective decline, measured via the MyCog and AD8 scales; RMT for faces and words; digit span forwards; BPVS; VOSP OD; Stroop; Camden PAL; digit symbol; Trails). Normality was tested using the Shapiro–Wilk normality test. After this, either parametric or non-parametric (Dunn’s test) post-hoc pairwise comparisons were used to investigated where differences were observed. Fishers’ exact test was used to compare the sex distribution between the groups instead of Chi-squared test as this is more appropriate for smaller sample sizes.
Behavioural performance on the VSTM task was compared between controls and patient groups. Due to a skewed distribution the absolute localisation error for each trial was log-transformed and analysed using a linear regression model. Analysis of object identity used a logistic regression model. Models used robust standard errors to account for clustering by participant. Regression analysis was used in order to allow analysis of the full trial-by-trial data which was available.
Visual exploration metrics and basic oculomotor characteristics, on each trial, were compared between controls and patient groups using multivariable linear regression models. Examination of residuals was performed to check model fits. For outcomes with skewed distributions (saccade amplitude, saccade duration, average saccade velocity, peak velocity, DT and Eq) bootstrapping, clustered on individual to account for repeated measures, was used to produce bias-corrected and accelerated (BCA) 95% confidence intervals (CIs) from 2000 replications.
To investigate the relationship between VSTM function and viewing behaviour we used multivariable linear or logistic regression models, where the outcome was the VSTM metric on each trial (identification accuracy or log of localisation error) and the predictors were group, sex, age at assessment, NART scores and the visual exploration strategy metrics (DT, Pr, Eq and S). Interactions were examined between visual exploration strategy metrics and group and between visual exploration strategy metrics, group and delay in relation to VSTM performance where relevant.
All models were adjusted for sex, age, NART and delay (1- vs 4-s). As saccade amplitude, velocity and duration are closely linked to one another, they were each included as covariates in corresponding models.
For each variable, participants were excluded if their overall performance deviated by 2.5 standard deviations (SD) from either side of the mean of each group (a total of n = 3 were excluded: n = 1 due to loss of eye-tracking signal throughout the experiment; n = 1 due to the DT score and n = 1 due to the Eq score). Statistical significance threshold was set to p < 0.05 and all analysis performed on Stata v.14.

Select A CommunityAllisonville MeadowsAllisonville Meadows Assisted LivingAmerican VillageAmerican Village Lincoln LodgeArbor Grove VillageAster PlaceAutumn Ridge Rehabilitation CentreAvalon VillageAvalon VillageBeech Grove MeadowsBeech Grove MeadowsBen Hur Health & RehabilitationBethany VillageBethany Village Assisted LivingBethlehem Woods Nursing & RehabilitationBetz Nursing HomeBrownsburg MeadowsBrownsburg Meadows Assisted LivingCanterbury Nursing & Rehabilitation CenterCardinal Nursing & RehabilitationClark Rehabilitation & Skilled Nursing CenterClinton GardensColumbia Healthcare CenterCommunity Nursing & RehabilitationCountryside Crossing Independent LivingCountryside MeadowsCoventry MeadowsCoventry Meadows Assisted LivingCreekside VillageCypress Grove Rehabilitation CenterDanville Regional RehabilitationEagle Valley MeadowsEast Lake Nursing & RehabilitationEastgate Manor Nursing & RehabilitationEdgewater WoodsElkhart MeadowsFairway VillageForest Creek VillageFranklin MeadowsGlenbrook Rehabilitation & Skilled Nursing CenterGood Samaritan Home & Rehabilitative CenterGreenwood MeadowsGreenwood Meadows Independent LivingHarcourt Terrace Nursing & RehabilitationHarrison TerraceHeritage House Rehabilitation & Healthcare CenterHeritage ParkHeritage ParkHickory Creek at ColumbusHickory Creek at ConnersvilleHickory Creek at CrawfordsvilleHickory Creek at FranklinHickory Creek at GreensburgHickory Creek at HuntingtonHickory Creek at MadisonHickory Creek at New CastleHickory Creek at PeruHickory Creek at RochesterHickory Creek at ScottsburgHickory Creek at SunsetHickory Creek at WinamacHillcrest VillageLake Pointe VillageLowell HealthcareMaple Park VillageMarkle Health & RehabilitationMeadow LakesMeadow LakesMeadow View Health & RehabilitationMonticello HealthcareMount Vernon Nursing & RehabilitationNorth Capitol Nursing & RehabilitationNorth Park Nursing CenterNorth Woods VillagePark Terrace VillagePrairie Village Nursing & RehabilitationRiverside VillageRiverview VillageRiverwalk VillageRosebud VillageRosegateRosegate Assisted LivingRosewalkRosewalk Assisted LivingRosewalk Village of LafayetteSalem CrossingSeymour CrossingSpring Mill MeadowsSpring Mill MeadowsSpringhill VillageSprings Valley MeadowsStonebrooke Rehabilitation CentreSummit City Nursing & RehabilitationSwiss Villa Nursing & RehabilitationThe Commons at Honey CreekThe Timbers of JasperTodd-Dickey Nursing & RehabilitationTrailpoint VillageUniversity Nursing CenterValparaiso Care & Rehabilitation CenterWashington Healthcare CenterWaters Edge VillageWest Bend Nursing & RehabilitationWestview Nursing & Rehabilitation CenterWilliamsportWilliamsport Nursing & RehabilitationWillowdale VillageZionsville MeadowsZionsville Meadows

Those struggling to communicate with a person who has memory loss are not alone. As many as four million people in the US may have Alzheimer"s, and, as our population ages, that number is expected to increase. Anyone who is a senior caregiver is likely to be affected and will need to understand how to cope with what is happening.
Memory loss associated with aging, dementia, and Alzheimer"s typically doesn’t happen overnight. Slowly, little-by-little, it sneaks up, until one day, family members realize that they can no longer communicate in the same way with the person they"ve known for years. They suddenly can"t rely on their words and their sentences don’t match the situation.
Because we cannot see the disease—the way we see a broken arm—it’s even more confusing when caregivers see how their patient and/or loved one will have good and bad days. The days when they’re alert and clear-headed make a caregiver hopeful. Then the bad days come, and family members and caregivers feel the pain of losing their patient and/or loved one all over again. This slow and normal progression of the disease makes communication a major challenge for caregivers.
There are strategies that caregivers can use to be more successful at communicating with someone who has dementia, Alzheimer"s, or memory loss. In the following video, nationally renowned presenter Diane Waugh shares dementia caregiver tips and strategies, drawing from her own experiences of being a caregiver for her mother:
Physiologically, dementia and/or Alzheimer’s affects various parts of the brain, specifically, it affects the brain in such a way that people have a difficult time learning new information. This is why, for a long time into the disease, patients and/or loved ones can remember things that happened a long time ago. They can remember wedding dates, the war they fought in, where they went to high school—but they can"t remember the visit that they had with their daughter yesterday. This is because the disease affects certain parts of the brain—the temporal lobes—which are responsible for helping us learn new things.
The reason they’re able to hold onto the memories that happened a long time ago is that those memories are represented throughout the brain. Long-term memories don"t require just one or two areas of the brain—they"re probably represented in multiple systems—so the disease has to be quite advanced before patients and/or loved ones start losing those memories.
In the brain of someone with dementia and/or Alzheimer"s, there are actual holes in the brain that form. In an image of an Alzheimer"s brain, one can see where many of the brain cells have died—and it affects every area of the brain.
The brain essentially has two jobs. The first is to make the best sense of what"s going on. Our brain wants to stay in control in every situation, and patients and/or loved ones with memory loss have trouble with that part: they want to be able to have some control, but they sense they’re losing some of that. The second job of the brain is to keep us safe—emotionally safe, as in, “I don"t want to fail,” or, “I don"t want to say things and have someone say, ‘that"s not right’.” Like any human being, we want to feel accepted and not ostracized or afraid to speak up.
There are three kinds of memories. The first is functional memory, essentially: reasoning and comprehension. This is conscious thought. When caregivers first see decline, it can be simple things such as: “How do I get from here to the grocery store?”, or, “How do I make the microwave work?”, or, “How do I balance the checkbook?” One of the places that family members may notice this decline in their loved ones is at restaurants: they will likely have problems trying to decide. They may say things like, “I’ll have that too” (indicative of a person unable to make a decision). They might say to themselves: “I don"t know what to do, so I’ll wait until one of the others at the table give me a sign that that’s what I’m supposed to do next.”
The second type of memory is procedural memory, or automatic memory. With these memories, there"s really no conscious control. This includes activities such as eating, driving or riding a bike—anything we"ve learned to do that is automatic.
The third kind of memory is emotional. This includes unconscious, gut reactions and are cued by something else that"s going on. This is where family members can help caregivers with their loved ones, because only family members know what types of emotions their loved ones have attached to certain things and/or activities (more about this under Communication Do’s).
Communicating with a person with memory loss can be difficult, but the right strategies can bridge the gap and foster a more fulfilling relationship between the patient and/or loved one. For caregivers—whether you"re a professional or a family member caring for a loved one—it’s important to adopt a positive attitude to effectively communicate.
Engaging with patients and/or loved ones in an encouraging and patient manner will help minimize feelings of frustration. If you"re struggling to connect with a patient and/or loved one with memory loss, it’s important to know a few common frustrations and “traps” and how you can avoid them.
First, remind yourself that people with dementia and/or Alzheimer’s only have the present moment, so we can let them know that we enjoy their company. When caring for someone who has the disease, the most important thing to take care of is that person’s feelings. A person with memory loss can’t remember the minute before, they don’t know what’s going to happen in the next minute. They can’t do that kind of thinking, so how they feel right now is the most important thing to pay attention to.
When you keep in mind that their feelings are the most important, arguments or resistance can be avoided. For example, maybe today you only help your patient and/or loved one with a half a bath or half a shower, and do the other half tomorrow, because right now, you can see they"re feeling tired and they’ve had enough. Keeping their feelings as the guiding light will help interactions go smoothly. Just think, “I want them to feel safe and/or respected,” or, “I want them to have a good time,” and it can make choices a lot easier.
A communication problem that can frustrate family members occurs when it seems as if the person with dementia and/or Alzheimer’s is lying. A typical example is a family member calls their dad and asks, “Did you take your medicine today”? Dad replies, “Yes.” But when the family member visits later, the medication is still in the package, and it"s obvious that Dad hasn"t taken his medication for days.
Communication problems can also occur around visits. A son may visit faithfully every night, but each time he arrives, his mother might say, “You never come to see me.” The son will feel that mom is purposely trying to give him a bad time. The person with dementia and/or Alzheimer"s doesn’t lay in wait, trying to hurt everyone’s feelings. It’s actually complicated thinking that the person with the disease can’t do. It"s important not to take what someone with memory loss says personally—he/she can"t always express your feelings accurately, and they aren’t even aware that he/she has hurt your feelings. Keep in mind that the person doesn’t remember that you visited yesterday. Rather than getting angry or frustrated, use the time together to do something enjoyable.
In addition, many older adults struggling with memory loss prefer familiar settings. In order to have the most productive interactions, arrange for visits to take place in a comfortable environment. Also, always begin visits by introducing yourself and defining your relationship. Quiet is key: silence any distractions, such as radios or the television. However, sometimes a change of scenery is in order. If you notice the patient and/or loved one is becoming agitated, suggest taking a walk or orchestrate a subject change. Refrain from negating the person"s emotions if he/she gets upset. Instead, offer acknowledgment and support.
Families may frequently ask, “Should I tell the person that he/she has Alzheimer"s?” Keep in mind that the patient and/or loved one can"t reason. They don"t have enough memory to remember the question, then think it through to form a conclusion. Caregivers and/or family members may often think if they tell the person with memory loss that he/she has Alzheimer"s, then he/she will understand and cooperate. You can’t get cooperation by explaining that he/she has the disease and expect him/her to remember and use that information.
A patient and/or loved one can construe even the simplest of conversation starters(“How are you today?”) as a real question, but they honestly don’t know the answer to it. This can be embarrassing and can send them back into a fog—they try their best to give an answer that makes sense to them and often produce immediate physical concerns: “I"m having a lot of pain,” for example. A caregiver and/or family member might ask, “What did you have for breakfast?” and the person with memory loss doesn"t remember at all. They might say earnestly, “I haven"t had anything to eat for weeks,” (because they honesty can’t remember the last time they ate). So these are questions to avoid because it causes fear for the person, that they have failed. But there are things you can talk about (which is covered under Communication Do’s.)
A patient and/or loved one with memory loss often shows progression in terms of their problems with language. The first sign is finding the right words for things, or word accuracy. The patient and/or loved one may be telling you something about a letter they received, but they can"t get the word “envelope” out, or they may point to a lamp and they can"t quite get the word “lamp” out. Language starts to become disfluent, and it’s difficult for the person to find the specific, right word that they want to express. Over time, their language becomes increasingly vague—it is more difficult for them to say something specific. For example, if you ask them what they do on a day-to-day basis, often they"ll say, “Oh, you know, I kind of do the same old thing. I kind of sit around a bit I do house things,” but they can"t offer specific details. This is because their store of language has become affected by the disease. In short, it is very difficult for them to express themselves in any great detail.
Another way to spot decline in language skills is substituting words. For example, they ask you to pass the salt when they meant to say sugar. Stop yourself from nitpicking them on accuracy: “You meant to say the sugar, so here’s the sugar.”Skip that whole conversation. You won’t teach someone how to talk, and, it can be construed as rude to ask that person to try a little harder, because they’re already functioning with half the brain cells. If they point at the sugar and ask for salt, just hand it over as if they said sugar. That’s the most respectful and kind.
People with dementia and/or Alzheimer"s may ask repetitive questions. Usually the question expresses a concern they have. Anyone with a concern that isn"t being addressed will become louder and more persistent. He/she may repeat the same question, because he/she cannot remember that he/she has just asked it, and their concern hasn’t gone away. It is the caregiver’s and/or family member"s responsibility to help soothe the worry. The goal is not to make the question go away—it is to make the worry go away for a little while, and then the question may come back. It"s perfectly okay to give the same answer again if it helps to calm the patient and/or loved one. Certain situations throughout the day will trigger repetitive questions—that"s to be expected.
People with dementia and/or Alzheimer"s may become aggressive in response to the environment. Bath time is often when the aggressive behavior is displayed. The caregiver’s and/or family member"s approach may also play a part. Rushing, speaking harshly, or forcing a person may result in an aggressive response. When someone with memory loss displays aggressive behavior, it is a form of communication. It may be the only way a person has left to say, “Pay attention to me! I don"t want to take a bath!” When someone is communicating vigorously, it is the caregiver’s and/or family member"s job to respect that communication. Hitting, kicking, or biting are ways of saying, “stop.”The appropriate response is to stop. That doesn’t mean not to try again in five minutes or a half an hour.
As strange as that may sound, learn how to enter into the patient’s/loved one"s world and not expect them to conform to our present day. As Diane Waugh, BSN, RN, CDP, says in the video above: “When I had to deal with memory loss with my own mother, I found the hardest thing for me to do was to not try to drag her into my reality, but to go live where she was living, in her understanding.”
Caregivers and/or family members should remember: give up expectations of the patient and/or loved one (who they were before in their life, for example, they always did all the bills, or, they always did XYZ as the go-to person). Giving up expectations can make room for what the patient and/or loved one"s strengths are (covered under Communication Do’s).
One of the biggest mistakes in dealing with patients and/or loved ones with memory loss is being negative and telling them that they can’t do something. Words like “no," “don"t,” or “can"t” create resistance. This comes up regularly with family members when the patient and/or loved one might be still driving, and the caregiver and/or family member has made the decision to stop them from driving. One should never say, “You can"t drive anymore.” They can still technically drive (they have the procedural part of the brain intact), and they can get very combative when told “no.” A way to counter this is to say, “I know you still can drive, that"s not even a question, but you know what happened the other day? I was out on the highway and this car cut me off, and I had to make a split-second decision it was really scary…” It’s likely they will say, “You know what? I"m having a little trouble with those decisions too.” The issue isn"t the mechanical driving, it has more to do with comprehension, and many times this answer works much better than, “You can"t drive anymore,” which can be construed as confrontational.
You may find a patient and/or loved one up too early or confused about time. Instead of using messages such as, “You’re up too early, you need to go to bed,” try leading with statements such as, “You know, I"m getting sleepy. I’d like a little snack before I go to bed,” and then gesture for the patient and/or loved one to sit with you.
It’s too final. Again, the patient and/or loved one is actually trying to make logical sense in their brain of why you are leaving, and they may get distraught and place the caregiver and/or family member in an uncomfortable situation. Instead, give a logical reason why you’re stopping the conversation, for example, “I"ve got to go to the store now and get my groceries.”
People with Alzheimer"s often ask difficult questions, mostly about people who have passed away years ago. It’s not helpful to remind the patient and/or loved one that a person they’re asking about has passed away. Rather than avoid the subject, you can say, “He/she’s not here right now, but tell me about him/her.” Often the person with memory loss is looking for the sensation and security that they would have if their loved one was around.
Caregivers and/or family members should be helping patients and/or loved ones comfortable, safe, and protected. Elderly women, for example, who have had children commonly ask, “Where are my babies?” This question will often come up at meal time, when feeding the children was an important part of motherhood. Find a way to soothe their concern. You could say, “The babies are sleeping.”
Sometimes memory loss is so devastating that we all forget that there is a person still in there somewhere. Family members can be distraught by what"s missing and forget that there"s still a lot there within the person, and that they have strengths.
They still have long-term memory, so it’s up to the caregiver and/or family member to “find them.” It"s interesting that, medically, doctors do tests on other conditions (pancreas, lungs, heart) but when it comes to memory loss, it"s often looked at like a switch: “Either they got it, or they don"t.” Just like everything else, there"s a progression of memory loss, and it’s up to the caregiver and/or family member to find out where the patient and/or loved one is, and bolster that.
Everyone has a short-term memory “drawer” and long-term memory “drawer”, and we put information in each. People with dementia and/or Alzheimer’s have a short-term memory drawer that has no bottom. He/she puts things in, and then they get lost. The long-term memory drawer, however, has a solid bottom. Lots of stories that are retrievable await (what he/she had for lunch in grammar school, for example). Encourage your patients and/or loved ones to tell you stories. You can even use photos to encourage stories. Photos are wonderful long-term memory reminders.
If the patient and/or loved one has a spiritual base, that is hardwired. A great example of this has been used to mitigate falls: if they know the adage of not allowing a Bible to fall on the floor, for example, you can put a Bible on their lap. That tells them, “I can work with you, I know you.”One can help patients and/or loved ones by playing to old spiritual memories: songs, Bible verses, poems that have a spiritual meaning. It can be very comforting to them.
Communicate with the loved one and/or patient by using the senses as conversation starters. What do they like to see? (Nature? Movies? Pets?) What do they like to smell? (Cake? Popcorn?) What do they like to taste, feel, or hear? Family members can help caregivers better connect and interact—offering just the simplest information on the patient and/or loved one, for example, “Oh, I know she loves the feel of cashmere,” or, “He loves to listen to birds.”These sensory preferences can also be used to help choose activities for people with dementia.
When words fail, body language can speak volumes. Touch is powerful, and many older adults are lacking in this valuable form of interaction. Holding hands, hugging, or even a simple pat on the back not only gives you a way to connect with your aging loved one, but can also help keep patients and/or loved ones engaged and focused. Eye contact is also critically important.
It"s not just body language that matters, however. Although the person with memory loss may be unable to express his/her feelings in words, keeping an eye on their body language can reveal feelings of anger, sadness, distress, or discomfort. If these occur, redirect the conversation to something more pleasant.
We all have different ways of communicating what we need, and people who have dementia and/or Alzheimer"s often don’t do well with verbal explanation. For example: “It’s time to take your bath, I"m willing to help you, let"s go.” It"s short-and-sweet, but the words fly right through. No matter what chore you’re wanting to address—the way to communicate it is often by not talking about it at all. Using gestures and eye contact can make a good-feeling connection to communicate what you need, without saying why or where.
Also, body posture is important. When we’re saying something to someone that we really care about, we tend to lean forward, we soften our posture versus sitting back and crossing arms and being more distant. Even late into the disease, a patient and/or loved one can understand body posture. They may not understand specific words, but they understand the context that the communication takes place in.
For effective communication, use a variety of cues. For example, to get the person to have a chair, you might pull up a chair beside the chair and sit down as you"re saying it, because that"s a typical social cue: when one person sits down in a friendly situation, the other person usually sits down. It just takes a physical cue and touching, then use simple words and simple phrases.
When communicating with someone with memory loss—even someone who has very impaired language skills—some very important things still get through. Even to the very end, the person can understand tone of language. Something that is said with a loving tone is understood quite a bit differently than something that is said with a harsh tone. The person with memory loss can catch those sorts of social differences in terms of use of language.
For some people, a distraction can be a good way to get the chore done. It’s kind of a different communication style that helps in distressing situations. For example, if a patient and/or loved one likes singing, starting him/her singing could allow the caregiver and/or family member to ease into bathing time with a gesture.
Singing actually can help tremendously with memory loss patients and/or loved ones who can no longer talk, or have trouble finding words to form sentences, because they are usually still able to sing a song. Often, they can remember the lyrics of a song from beginning to end.
Many patients and/or loved ones can still read as well. Singing and reading can give the person great joy and hearing a loved one’s voice can very comforting for family members.
Using “I” messages along with an enjoyable distraction and gestures is more effective than “you” messages. For example, “I was thinking we could have a snack,” and gesture to the table and the food. Avoiding “you” messages makes exchanges more pleasant—there is no pressure on the patient and/or loved one to look for answers that are no longer retrievable.
Patience is an essential part of communicating with a patient and/or loved one with memory issues. Offer a prompt if he/she is struggling to find a particular word, but make sure you are open to listening—even if it takes longer for them to reply.
Family members may frequently ask, “How often should I visit?”, or, “Should I visit at all, because they don’t seem to be understanding what we’re saying, most of the time they don’t seem to recognize me, etc.” Caregivers can encourage family members to visit because it’s important to them. Also, the person with memory loss may catch some things on some days, and if family members can make the interaction a pleasant moment, it can be rewarding for both.
Communication amongst family becomes particularly difficult when the person with dementia and/or Alzheimer’s doesn"t recognize family members anymore. In this situation, a spouse or children can think that it doesn’t do any good to go talk to the person—that anyone could talk to him/her because they don’t remember who they are. But there is a richness that happens because of fami


 Ms.Josey
Ms.Josey 
 Ms.Josey
Ms.Josey