
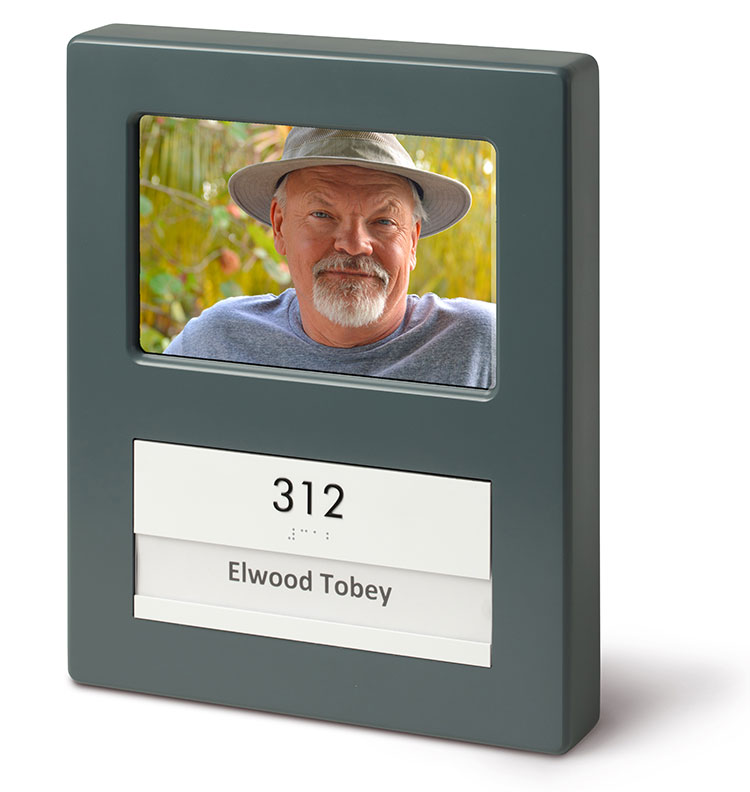
display screens for memory impared supplier

A screen magnification system enlarges text and graphics on a computer screen. It is loaded into the computer’s memory and functions similarly to a magnifying glass moving over a page, following the cursor, and magnifying the area around it. Using a mouse or keyboard commands, a user positions the cursor on the section of the screen to be magnified or has the cursor move automatically across and down a magnified page at a preset speed. The magnified area may also be emphasized with color and shading, so that users who lose their place on screen may easily locate a magnified area. Fonts used in magnification programs are usually designed to smooth out the jagged or “stair-step” appearance of computer-produced diagonal or curved lines. Today’s full-featured screen magnifiers can magnify all items on a screen, including the mouse pointer, text cursor, icons, buttons, and title bars. The magnifiers also provide a set of mouse tracking features.
Persons with considerable vision may not need a screen magnification program. Instead, they may use a larger monitor that allows for larger text or graphics while keeping all material on the screen. Larger text and graphics can be achieved by lowering the screen resolution so that bigger pixels are used.
In addition, the appearance of objects or texts on a screen may be altered using the accessibility wizard in a Windows system, which provides a number of options. These options include adjustments for the font size, screen resolution, scroll bar size, icon size, color scheme, mouse cursor appearance, and mouse cursor blink rate. The main accessibility feature in Windows, however, is its screen magnifier which can also be set up through the accessibility wizard. Although the default color scheme in Windows is black text on a gray background, this can be changed to be more easily distinguished using one of Windows high-contrast color schemes.
Portable battery-operated and braille-compatible screen reader and scanner with a built-in screen for displaying photos, magnifying small objects and enlarging texts for individuals who have difficulty reading printed text.
Lightweight, battery-operated, portable scanner and reader that comes with a pair of headphones that easily plugs into the front of the device for privacy. The ergonomic thumbwheels and tactile controls are intuitively located for ease of use. Braille-display compatible for reading a book or a menu at a restaurant or filling out a form at the doctor"s office. Incorporates the AudioMinder technology, allowing the user to set an alarm and record appointment reminders.
Fast, accurate, and easy-to-use scanning and reading appliance that connects to a monitor or TV to display text in a high-contrast, large font so user can read along as the content is spoken. May be used for scanning a printed page, pill bottle, recipe card, or newspaper. Motion detector automatically senses when a new page is placed under the camera.
Screen magnification and screen reading software for Mac users. Provides magnification, contour enhancement and pointer settings as well as screen reading with high-quality speech output. In addition to text to speech voices, such as Infovox iVox by Acapela, it comes with automatic language identification in the screen reader mode and GhostReader, an application for reading documents. GhostReader contains shortkeys for fast and easy access to the text and the user can listen to documents including file types such as Text, Word, HTML, PDF, ODT or RTF. Also allows user to save texts as Mp3-files to be played in iTunes, be uploaded to an iPod, iPad or burned onto a CD.
Compact and portable lightweight reading device that scans and reads text documents such as books, newspapers or bills with a push of a button. May be connected to an external monitor via VGA and HDMI connectors and has 8 zoom settings. Offers fully readable letter size with an option for column recognition and allows documents to be stored for later use. Has a standard audio jack for headphones or external speakers. Internal battery available for portability.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices. Allows users to write map files to make nonstandard applications usable.
Combined screen reader and magnifier that allows users to access Windows applications either through magnification, braille, or speech output. Computer display is magnified up to 64x and the information is also presented in braille for users of the many supported braille devices.

I can’t thank you enough for working me to get the phone up & running for my mom. She’s starting to adjust to using it. This phone will help her as she gets flustered with all the options even on a basic cell phone.
I am so grateful for this phone & the wonderful support staff that helped me with my questions & missteps. Tried out the phone with family members & are anxious to give it to her on Monday, her 92nd birthday. This will be a godsend for her to be able to communicate with her family during these difficult times. Usually there are only 5 stars but would give 10! Thank you for making this a very bright moment. Thank you again.
I have been looking for a phone that would not confuse my Mother with her dementia. I have not found a phone that would work for her until I found this one. Having the ability to set up and control the phone from the caregiver portal has greatly reduced the time I have to spend dealing with phone issues. My Mother lets me know if she needs to add a number to her list and I can do the from anywhere without having to physically change it on her phone. I also like being able to check the battery level from the portal adn let her know if she needs to charger her phone if she forgets. No more assuming the phone is just dead. The GPS feature also gives me peace of mind to know were she is or if her phone was left somewhere. This is a great solution if you are looking for a phone for your family member with dementia.
I am so very thankful for this phone. It has given my father a sense of freedom again. His confidence in using the phone is phenomenal and we haven’t been able to say that in a while. I am wondering if there is a case that can be recommended that has a cover for the front that will stop accidental calls. PLEASE LOOK AT THIS PHONE FOR YOUR LOVED ONE, YOU WON’T REGRET IT.
I purchased this phone for my mom who has dementia and was having great difficulty using even her simple flip phone. It is very easy to use and wonderful that I can manage the phone from the portal. I would rate “5” except 1) I assume there is no way to disable the 911 function due to legal issues, but it would be nice if I could since she is in a nursing home and help is always nearby; 2) would be nice to get rid of the message that says “individual’s voicemail has not been set up” since there is no voicemail option (I get calls from my mother’s family asking why she has no voicemail); 3) would be nice to be able to increase the number of rings. It only rings four times and it usually takes her longer than that to get across her room to answer since she doesn’t carry the phone around with her. All in all, though, very happy with this purchase.
As for 2) the voicemail message and 2) the number of rings – these are control day the wireless provider. The number of rings / ring duration can bu adjusted by some of the carriers. Please contact the carrier and request it to be changed.
This phone is very nice to look at and easy to use. I love that we can limit the calls that my mom receives. She was always so confused by the spam calls about the extended warranty for her car. It’s great that she doesn’t get those anymore. It’s also really nice that she can see photos of my sisters and me to decide who she wants to call.
However, there are a couple of things I do not like. One, the volume is fixed, and it is too loud for certain situations. Secondly, there is no way to track missed calls, or voice mail.
This phone solved our conundrum with needing a simple phone for our older guy who now feels reconnected without the barrage of incomprehensible scammers. The tech support and customer service is responsive, efficient and superb.
I just wanted to say thank you for this product. My mom, who has dementia, broke her hip, got COVID while in the hospital and ended up recovering from both in isolation in a nursing facility. She has been struggling to understand what is happening to her and not being able to be there with her has been a challenge for all of us. This phone has helped her tremendously. She had forgotten how to use a cell phone a long time ago but she can use this phone and it has lifted her spirits to stay in touch and she likes looking at our pictures. It’s such a well designed product and the customer support you offer is very appreciated as well. The staff at the Verizon store wrote down the information because they said they get requests for senior-friendly phones all the time and they don’t sell anything like this phone. The therapy staff at the nursing home commented that they love the phone as well and will be recommending it to other families in the facility.
This phone has been a godsend to me as the caretaker of my mother from three states away. I love how I can manage the phone via the portal. There are so many things I love about this phone and its ease of use for my mother. Other reviews talked about the default ringtone volume being very loud and unable to change. The ringtone volume was super loud! I called RazMobility Support and they walked me through how to lower the ring volume (but you can only do it when having the phone physically with you and they walk you through all of the steps). I’m sure there are other changes RazMobility support can help you with. Just call them and ask, “Can _____ be adjusted on the phone?” They have been super helpful. I love how simple the portal is to manage and how I can see the battery life, and GPS location of my mother’s phone. The MintMobile cell service did not do too well in my mother’s nursing home, but it was easy to switch out the SIM cards to another carrier. But make sure you purchase the more expensive Raz phone so you can easily switch carriers if you need to. I would have stayed with MintMobile if the reception was better as their website is super easy to navigate. So this review doesn’t go on forever, I’ll focus on some features I would like to see in the future: recent call list, ability to adjust the ringtone volume, voice volume from portal. One glitch I’ve found is that when my mother presses the “Hang Up” button too long, she accidentally calls the contacts listed in the #5 & 6 spots. To avoid her accidentally calling someone a lot, I added my contact info into slots 5 & 6. So if it happens, she is just calling me. We also bought the wireless charger (which comes with the protective phone case). That way my mom does not have to struggle to plug in the regular phone charger. The wireless charger charges super slow to avoid wearing out the battery. This phone is awesome. Raz, if you created an affiliate program, I think you could get the word out even more about this phone. I would be a huge cheerleader of the phone!
I purchased this phone for my Dad who we just moved into a nursing home due to dementia. He became unable to remember how to work his old cell phone or the regular telephone. The RAZ has been a Godsend. It’s so easy for him to use and he is absolutely thrilled to be re-connected with his family. I had a little trouble activating it, ( a senior citizen setting up a phone for a senior citizen…what could go wrong???). But I called customer service and the rep that helped me was amazing. Patient and knowledgable and even emailed me pictures of what things should look like along the way. She made sure I knew how to add names and pictures to the phone and even offered to do it for me if I emailed her the pictures. I’ve called a few times with questions and I reach a human being quickly and they always know the answer to my questions. Customer service of the highest caliber. So far the only downside is that when the phone is in the case the volume of the ringtone is very low and my Dad doesn’t always hear it. I’ve called customer service and they told me that I have to be near the phone to adjust the volume, so the next time I am there I will give them a call. The RAZ is the absolute perfect cell phone for any senior but especially one who has impaired mental capabilities.
My 92 year old father loves this phone. I love not worrying that someone is scamming him over the phone. He loves showing it off to his friends at the retirement community. I love not spending hours trying to talk him through getting him back on his phone. He loves not calling the wrong person because he touched the wrong line in his contacts. I love updating new phone numbers for his contacts without having to have his phone in hand. For us it’s a win/win/win
My Dad doesn’t have dementia but is 87. We got the Raz phone and it’s like a long, cool drink of water. We tried Jitterbug and Jethro “senior friendly” phones and they were a JOKE. Raz is the first truly SIMPLE phone – no menus, God bless them, and remotely configurable. The only thing I would criticize, and I hope Raz is listening… About once or twice a day, the Raz phone makes an outgoing call while in my Dad’s pants pocket. I have witnessed this first-hand. He’s puttering around the kitchen, not bending over, not with his hands in his pocket, and his phone calls me. If he were allowed to “turn off” the screen before he puts the phone in his pocket, I believe the problem would be fixed. We did try a belt holster, but with his posture, his belt is too close to his armpits and it takes so long to get the phone out of the holster that the phone stops ringing before he can answer.
I purchased this phone for my brother who has rapid arm and hand tremors due to Parkinson’s Disease. He also has early Dementia. He is not tech savvy at all. The Raz phone is truly a blessing to him and my family not only because it’s simple and easy to use, but it eliminates the clutter he would have to navigate through using the traditional smart phone. He is proud that he has a device that is fully simplistic and streamlined to his need, but also instills his dignity just by the phone’s impressive appearance. Raz mobility technical support is Fantastic! I have dismissed products from other companies just on the premise of customer support alone, regardless of the quality of product. I was helped by Alex at Raz Tech support. He was extremely knowledgeable, methodical, courteous, and above all, patient. I enjoyed one of the best customer experiences I have had in many months. Kudos to Alex.
I found the RAZ Phone easy to get set up and it works as advertised. This will be a big help as my wife has memory problems. Now I feel comfortable being away from her for a while. Thanks.
Great phone for those with dementia. Easy to set up from the caregiver portal. Customer Service is great. An improvement would have the phone shut off automatically if not being used since the battery goes down and the phone has to be charged daily.
I recently returned my mother’s Memory Cell Phone because someone at her care facility had inadvertently exited the app and did a factory reset. Within a week, I had the phone back with the app reinstalled. Not only that, you installed the new version which has great new options AND sent a complimentary wireless charging platform because she had damaged the charger port trying to put the charger in the wrong way. That is customer service above and beyond.
This is close to being the perfect phone for those with dementia and those of us who care for them. It is so very well thought-out, anticipating all the problems. For the first time in months, my husband can call me when he’s feeling anxious or worried from his memory care facility. It has been such a relief for both of us.
The Memory Phone has been a wonderful solution to our parent’s dementia challenges. What a relief to have the confidence that they can call when they want and not be discouraged by the complexity of a smart phone.
The RAZ is a great phone. Customer service is outstanding. I bought this for my Mom who has Alzheimer’s. Unfortunately we waited a little to long to make the change. She was not able to make the adjustment to the phone and I had to return it. With that being said, this is a wonderful cell phone, I am super impressed with how it works and the options for the caregiver from the portal. I will be telling anyone I know who needs this service. We did the T-Mobile version and had zero problems. Just put the SIM card in and it worked perfectly. Thanks for a great product!
RAZ MEMORY phone is exceptional for my father in law age 94. He has some age related dementia combined with macular degeneration. Especially helpful are the auto answer to speaker phone options. He is able to call us usig the limited photo buttons. And, NO MORE JUNK CALLS. Wish we were aware of this earlier. We are showing it off at his new Assisted Living Community. We also love the optional charging cradle which is home for the phone most of the time.
This phone is fabulous for my mom who has dementia. We tried several ‘easy’ and ‘senior’ phones before finding this one. This is the only one she’s been able to use reliably. Being able to control the phone settings from my phone is great; no more deleted contacts or turning her phone off then wondering why it wasn’t working. The phone works well on the T-Mobile network. I had to contact customer service and was shocked to be connected to a person right away. He immediately identified the issue and walked me though how to fix it. The call lasted maybe 5 minutes and there have been zero issues since. I wish we’d found this phone a couple years ago. It would have saved both mom and family members a lot of frustration.
Easy for my non-tech husband to use. We set it to auto answer and speaker phone, so he doesn’t even need to pick it up. Makes us feel more secure for those times when I need to leave him alone for short periods.

This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data.

The information on this website is for general informational purposes only. No information contained here should be construed as professional medical advice. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking treatment because of something you have read on this website. References in this website to any third-party products, services, processes, hypertext links to third parties or other information by trade name, trademark, manufacturer, supplier or otherwise does not necessarily constitute or imply its endorsement, sponsorship or recommendation by Soo Borson or the administrator(s) of this website. Links to other websites are provided for your convenience and Soo Borson and the administrator(s) of this website disclaim any responsibility for the content, accuracy of the information and/or quality of products or services provided by or advertised on these third-party websites.
Screening for dementia, much like screening for other diseases or chronic conditions, is a good way to detect the changes that can be signs of the onset of disease or other change in cognition. Memory screening and early detection provide:The ability to make lifestyle and other beneficial changes earlier in the disease process when they have the greatest potential for positive effect.
Time to connect with community-based information and supportive services prior to a potential crisis situation related to the needs of the person with dementia or the caregiver.
To enable people with dementia and their caregivers to benefit from memory screening and early detection, a community-based memory screening program was developed by the Wisconsin Department of Health Services and the Wisconsin Alzheimer’s Institute using the Animal Naming Screen, the Mini-cog, and the AD8.
The Animal Naming and Mini-cog tools were selected after a pilot study in Portage County in 2009. The Wisconsin Alzheimer’s Institute, the Aging and Disability Resource Center (ADRC) of Portage County, and DHS demonstrated the acceptability and effectiveness of using the Animal Naming and Mini-cog screens in a community setting. The Animal Naming screen is attached as Appendix C (PDF) and the Mini-cog as Appendix D (PDF)
Results from the pilot demonstrated ADRC customers’ high level of acceptance of screening. The offer of a memory screen was accepted by 243 out of 254 people, a 96% acceptance rate. This result contradicts the idea that people do not want to be screened for dementia. The tools were also effective in detecting cognitive issues. Of the 243 people who were screened, 150 (63%) had results that indicated they should follow up with their physician. This result may seem surprisingly high, but screens were only offered to individuals who expressed a concern about their memory, so those with cognitive issues self-selected into the study. Of those 150 people, 120 or 80% agreed to have the results sent to their physician.
The Animal Naming and Mini-cog screens were selected not only for their acceptability and effectiveness, but also because they are brief, easy to administer and score, and are sensitive to early cognitive changes. Some screens must be administered by physicians or psychologists and can take more than an hour. The minimum level of training required and the short length of time necessary to administer the screens was a critical component in their acceptance for use by ADRC staff.
The screens were also selected because they have documented utility as dementia screens and tap key skills likely to be affected in mild to moderate dementia. The Animal Naming screen involves retrieval from semantic memory and executive function, two areas of cognition that reliably decline in people with Alzheimer’s disease. In a study of memory clinic clients with a high base rate of dementia, the Animal Naming screen was shown to have 85% sensitivity and 88% specificity for differentiating Alzheimer’s disease and other dementia from normal cognition. The Mini-cog screen tests memory as well as visuoconstruction and executive function, with studies showing sensitivity for dementia of 76% to 99% and specificity of 83% to 93% in analyses that excluded patients with mild cognitive impairment.
Memory screens are voluntary, so there will be individuals who decline to participate. On these occasions, if family caregivers are uncertain whether their concerns about the person they are caring for are valid, the AD8 screen can help determine whether a visit to the doctor is recommended. The AD8 (PDF) tool is available in both English and Spanish. This screen is intended to help the caregiver think through the changes they see in a family member, and may help them to realize it is time to take action. The screen can be provided to the family caregiver to complete on their own, or the questions can be asked by the screener in a private setting. The AD8 has sensitivity for dementia of greater than 84% and a specificity of greater than 80%.
In 2020, the Montreal Cognitive Assessment (MoCA) tool was added to the approved tools for use by dementia care specialists (DCS). This tool is not for use by ADRC staff other than the DCS. The intention behind the addition of the MoCA screen is to give DCS an additional tool for situations that are more complex. While the Mini-cog and the Animal Naming screens are more sensitive to earlier changes than other screens, they are limited to a few areas of cognition. The MoCA covers a wider variety of cognitive tasks and provides additional insight into possible cognitive impairment when the Animal Naming and Mini-cog results do not reflect the changes in cognition and behavior reported by the individual or their family.
New dementia care specialists should become very familiar with the Animal Naming and Mini-cog tools prior to adding the MoCA to their toolkit. There are some similarities and some differences between the activities of the Animal Naming and Mini-cog and those in MoCA. Learning all the screens at the same time can be confusing, so it is advised for new staff to focus on the Animal Naming and Mini-cog screens, as well as the AD8, prior to becoming certified to provide the MoCA screen. Training and certification for the MoCA, and the approved form, are available from the official MoCA website. There is a cost to the training and certification for the MoCA. The MoCA is not required to be provided as a part of this program but is available as a supplemental tool.
The primary intent of this memory screening protocol is to enable and enhance conversations about memory concerns. The screens are not diagnostic tools and do not make any determinations about mental status. The screens are similar to a blood pressure check, in that a high blood pressure reading does not mean an individual has cardiovascular disease, but is a signal to talk to a physician about the results. The screens can be a reason to bring up the topic of memory issues because they can be offered in the moment. A referral to the physician can be more meaningful if an objective tool verifies that an individual’s concerns with memory and cognition should be further assessed.
It is appropriate to offer a memory screen when one is requested, or when working with a customer who displays signs of possible memory loss or confusion. ADRC specialists are able to offer the screening program during a visit for another purpose, if time allows. It is preferable to address the concerns around memory at the time, rather than putting off the discussion for another appointment. Memory screening is always voluntary.
Staff members may feel uncomfortable offering a memory screen if they are not used to asking and answering questions about memory and dementia. It is important that staff who are offering the screens understand why screening is important and helpful to the customer. Practicing offering the screen to coworkers and family members can be a good way to become more comfortable. Staff must be trained to follow the guidance in this manual before performing memory screens with the public.
If other people are present for the screening, let them know they will need to remain quiet and not help the person answer the questions. Ensure the participant cannot easily view and copy a clock in the room.
Begin with Animal Naming. It is critical to read the instructions for each task on both screens exactly as they are written. Do not explain how the screen is scored prior to performing the screen, and only afterwards if the individual asks you to do so. To adhere to the fidelity of the tools, they must be performed exactly the same way every time to ensure the results are valid. Read the instructions to the participant: “Please name as many animals as you can think of as quickly as possible.” Be prepared for the person to start listing animals immediately or, if they do not, prompt them with “Go.”
Once the person begins to name animals, start the timer and record all the animals named within 60 seconds in the spaces provided on the worksheet. If the person is speaking quickly, write as much of the word as needed to remember what was said and fill in the remaining letters afterward. If the person falls silent, follow the prompting instructions. Once the Animal Naming screen is done, administer the Mini-cog, even if the score of the Animal Naming screen was very high. The two screens should always be used together.
The Memory Screening in the Community program is intended for the Animal Naming tools and the Mini-cog tool to be used in combination. In this non-clinical program, the standard Mini-cog tool available online has been adapted to work in concert with the Animal Naming Tools. Refer to Appendix D to access the form to record results.
Begin the Mini-cog by telling the participant, “I am going to say three words I want you to remember,” and repeat the three words listed on the worksheet. Be sure to read the instructions exactly as they are written. It is important to the fidelity of the screen to use the same three words every time the screen is performed. Give the participant three chances to repeat the words back. If the participant does not repeat the words, or does not repeat them correctly, the screener can repeat the words up to three times until the words are repeated correctly. If they are not correct after the third time, move on to the clock draw.
Provide a blank, standard, letter-size sheet of paper for the participant to draw on and a writing utensil. This can be the back of the Animal Naming worksheet or another blank sheet. Allow the participant time to adjust to the new task, pick up the writing utensil, and adjust the paper. Once the participant is settled, read the instructions for the clock draw exactly as they are written, pausing when indicated to allow the participant to complete the task. Move on from this task if the clock is not complete within three minutes.
There will be individuals that frequently request to be screened. If they express the desire for an alternate set of words used for the three-word recall portion, refer to the words listed in the Health Equity section for Hmong translation. The need for an alternative set of words was first identified in the need for the translation of the words into Hmong. they do not easily translate into that language, so an alternative set of words was identified for that purpose. That substitution can also be applied for individuals who request frequent screening.
The AD8 can be administered to the person with possible memory loss, but often individuals with dementia lose insight into their condition and are not reliable self-reporters. The questions on the screen can either be read aloud or a caregiver can fill out the form on their own. In situations where the person with possible memory loss is together with the caregiver, allowing the caregiver to fill out the questionnaire silently may be less upsetting for the person with possible memory loss than if the questions are asked aloud. The caregiver may also provide different answers if the person with possible memory loss is listening to the answers.
The MoCA tool, including training, certification, and the downloadable version of the paper tool can be found on the MoCA website. The MoCA is also available to be used digitally. Instructions for how the MoCA tool is scored are a part of the training and certification process.
The Memory Screening in the Community program was adapted in 2020 during the COVID-19 pandemic for use when screening was required to be completed virtually. The ability to provide screening virtually for dementia risk has been identified as an ongoing need. Please consult Section IV: Accessibility and Health Equity Considerations for a description of the adaptation for virtual access.
The use of the Animal Naming and Mini-cog tools in the Memory Screening in the Community Program is different than as a part of Wisconsin’s Long-Term Care Functional Screen (LTCFS). The purposes for the use of these tools in the Memory Screening in the Community Program are to enable a conversation and assist in determining whether speaking to a physician is advisable. The LTCFS uses the tools to represent “memory loss” if the individual being screened states that they have memory loss but do not have an accompanying diagnosis of dementia. The LTCFS is used to determine functional eligibility for long-term care programming and uses the results of the screens independently. The scoring key for the Memory Screening in the Community Program to determine if a referral is recommended is attached in Appendix E.
The Animal Naming tool is a categorical fluency test. The person is asked to recall specific labels for items in a specified category, such as animals. The tool is scored by tallying the number of correct responses. If the person names fewer than 14 correct animals, that is considered “not passing.”
The Mini-cog has two areas that are scored. Three points are awarded for recalling the three words correctly, and a score of either zero or two is awarded for the clock draw. For the three- word recall, one point is given for each word remembered. The words do not have to be in the same order in which they were presented.
The clock draw test requires some interpretation by the screener. The rules for scoring the clock draw are attached inAppendix G. There are examples of clocks drawn by participants in the pilot study that can be used to practice interpreting results in Appendix H. It is important not to overthink the interpretation of the clock; the clock is only one piece of the screening program. If a clock drawing looks correct but there are some questionable features, use your best professional judgment to make a decision and then move on.
The screens are conversation tools and do not provide a diagnosis; they are used to determine the need for an appropriate referral to a physician. If the scores from the screens do not indicate the need to make a referral to a physician, but the conversation about the individual’s memory concerns suggests that a referral would be helpful, a referral should still be offered.
The AD8 is scored by tallying the number of items noted as “Yes, a change.” If the score is two or more, a referral to the physician is appropriate. The instructions for determining the score of the AD8 can be found after the screening questions on the AD8 tool.
Training for the scoring of the MoCA tool can be found on the MoCA website. The MoCA is available to be used digitally, which can assist in scoring the results.
The screener can also offer to send in screening results for individuals whose scores do not fall into the range where a referral is recommended for the purposes of providing a baseline screen for their medical records. A baseline score is useful in detecting change over time. If an individual has several years of baseline scores in his or her record, detecting a change in cognitive abilities is easier to track and therefore easier to detect and respond accordingly.
If the person who was screened chooses to have the screening results shared with a physician, the screener must first obtain a signed ‘release of confidential information’ form giving permission to the screener to share the information. An example of this type of form is located in Appendix I, although most agencies will have their own form that must be used for this purpose.
Sending the screening results to the physician is also an opportunity to make the physician aware of the agency and its services as well as the community screening program. Cover letters should include information about the person who was screened, a short explanation of the screening process, information about the agency and a statement encouraging the physician to refer patients who receive a diagnosis back to the agency for ongoing support. A sample letter to the physician is attached in Appendix J.
The Wisconsin Alzheimer’s Institute (WAI) and the dementia care specialist from Eau Claire County developed additional resources for use after the tools have been completed. For individuals whose screening results show they should talk to their doctor, Dr. Cindy Carlsson at the WAI developed a one-page document to accompany screening results sent to the physician by the screener. The document includes best practices around evaluation for possible dementia and when to refer a patient to the WAI Memory Diagnostic Clinics network. This resource can be found inAppendix K. Appendix L is the Memory Screening Results and Recommendations form available to provide the person after screening and is optional. Having the results and recommendations written in one place can be helpful to the person. Additional information and resources can be provided at the time or sent in a follow-up correspondence.
Once the tools are completed and a physician referral is recommended, the screener should ask permission to follow up after two to six months, even if the individual does not want the results sent to the physician. Agreeing to a follow-up call indicates openness to additional support in the future. If the person who was screened does indeed have dementia, they will need information and support in the future, and following up after a screen can allow that to happen in a planful way and not in crisis.
The Memory Screening in the Community Program can be provided in a variety of settings. Typically, screens are available whenever a customer requests a screen, or when a trained ADRC specialist or dementia care specialist identifies a customer that would benefit from the program. They are also usually performed in person. This can be during a home visit or office visit scheduled for another purpose. However, there are many possible locations for memory screening to be performed in the community. Partnering with municipal and other local governmental agencies to offer screens is one option. For example, public libraries are welcoming places free from the stigma associated with dementia and are often willing to host screening events in a private study room or other private space. Community or large employer health fairs also offer opportunities to screen, and to normalize screening for cognitive decline along with other health conditions.
County-based programs, healthy aging programs, public health departments, and other community-based partner agencies may also have staff trained and supported by the dementia care specialist at the ADRC to provide the Memory Screening in the Community Program. The same requirements for fidelity, oversight, and yearly refresher training apply to all screeners trained by the DCS.
The Memory Screening in the Community Program was adapted during the COVID-19 pandemic to be available virtually. When the program cannot be provided in person, there is a substitute protocol for use of the program virtually. Please consult Section IV: Accessibility and Health Equity Considerations for a description of the adaptation for virtual access.

The Saint Louis University Mental Status (SLUMS) ExaminationThe SLUMS examination is brief test designed to measure a patient’s abilities in orientation, executive function, memory, and attention. Evaluation of the exam can be used to determine if a full-diagnostic assessment is needed.
General Practitioner Assessment of Cognition Screening Test (CPCoG)The General Practitioner Assessment of Cognition Screening Test is a cognitive impairment screening tool designed for use in primary care.
Memory Impairment Screen (MIS)The MIS is a quick screening tool to assess memory. It can be used as a preliminary screening test, or in conjunction with other screening tools to evaluate the cognition of a patient who has exhibited possible impairment in their thinking and recall functions.
AD8 Dementia Screening InterviewThe AD8 Dementia Screening Interview is an eight-question interview, which distinguishes individuals who have very mild dementia from those without dementia. This tool is based on individual decline and is a valid and reliable screening tool for dementia. Its use is granted by Washington University for clinical care purposes in family medical care.
Mini-Mental State Examination (MMSE), 2nd Edition™The Mini-Mental State Examination, 2nd Edition™ application allows users to administer, score, and share patient results faster and easier than using pencil and paper assessments. The application is available for smartphones and tablets, and there is a fee associated with using the tool.
Although this may sound like the obvious and simple solution, my friends who are primary care providers remind me that they barely have time to do the basics — like blood pressure and diabetes management — and that they have no time to administer fancy cognitive tests. Even a simple test like the Mini-Cog (clock drawing and three words to remember) is too long for them. So how are we going to diagnose the increasing numbers of individuals with Alzheimer’s and other dementias in the next few decades?
In 2010, clinicians at the division of cognitive neurology in The Ohio State University Wexner Medical Center developed a cognitive test to screen for memory loss that individuals can self-administer. This concept of a self-administered cognitive test can solve the problem of the time-crunched primary care provider. Individuals can take this test in the privacy of their own home and bring the results with them to the office. The results can then be used to determine whether additional work up and/or referral to a specialist is indicated.
To answer this question, the authors performed a retrospective chart review on 655 individuals seen in their memory disorders clinic, with a follow-up of up to 8.8 years. They compared their SAGE test to the MMSE.
Based on both initial and follow-up clinic visits, they divided their clinic population into four groups. Before I describe the groups, let me explain a few terms:
Even a self-administered test that individuals can do at home will still require training for primary care providers, to understand how the test should be used and how to interpret the results. There is no question, however, that such training will be worthwhile. Once the training is complete, the knowledge gained should be able to save literally thousands of hours of clinician time, in addition to missed — or improper — diagnoses.
Another question is how individuals will react when they are told that they need to perform a 10-to-15-minute cognitive test at home and bring the results to their doctor. Will they do it? Or will the ones who need the test the most avoid doing it — or cheat on it? My suspicion is that people who are concerned will do the test, as will people who generally follow their doctor’s instructions. Some individuals who would benefit from the information that the test provides may not do it, but many of those individuals wouldn’t do the "regular" pencil-and-paper testing with the doctor or clinic staff either.

: A telephone battery was administered that included the Memory Impairment Screen by telephone (MIS-T, a test of semantic memory), the Category Fluency Test (CF-T), and the Telephone Instrument for Cognitive Status (TICS). An in-person evaluation then followed that included a neurological examination, a neuropsychological battery, demographics, and medical history.
: The telephone battery was well accepted. The MIS-T required 4 minutes; the CF-T, 3 minutes; and the TICS, 10 minutes. The MIS-T had excellent sensitivity and specificity when compared with the CF-T and the TICS. Using cutscores on all three tests that provide a sensitivity of 78%, specificity was significantly higher for the MIS-T (93%) than for the CF-T (78%, P<.05) or the TICS (80%, P<.05). Combining the MIS-T and CF-T improved discriminative validity but increased screening time and the complexity of scoring. Normative data for the MIS-T, the CF-T, and the TICS for use in settings with different base rates (prevalence) of dementia are presented in this study.
: The MIS-T outperforms the CF-T and the TICS as a valid and time-efficient telephone screen for dementia. For applications that require optimal efficiency and accuracy, the MIS-T is recommended.

The memory impairment screen (MIS) is a brief screening tool to assess memory. It is often used as a preliminary test, along with other screening tools, to evaluate the cognition of someone who seems to display some possible impairment in their ability to think and recall.
The MIS is one of three tools recommended for use in the Medicare Annual Wellness Visit by the Alzheimer"s Association. The other two are the GPCOG and the Mini-Cog.
Four words in large print (24 font or larger) are shown to Maude and she is asked to read each item aloud. For example, the four words may be checkers, saucer, telegram, and Red Cross.
Maude is then given a category and asked to identify which word fits that category. For example, the category of "games" is provided and she must be able to identify that the word "checkers" fits that category. After completing this task for all four words on the paper, the paper is removed from sight and Maude is told that she will have to remember these words in a few minutes.
Next, Madue is asked to perform a task that distracts her from the four words she just learned, such as counting to 20 forwards and backwards or counting backwards by sevens starting at 100.
If more than 10 seconds have passed with no words recalled, Maude is then given the categorical clue for each word and asked to recall the word. For example, the test administrator will say that one of the items was a game and this might prompt Maude to remember the word "checkers." This is the cued recall section of the test.
For each word recalled without any clues (free recall), Maude will receive two points. For each word recalled with the categorical clue, Maude will receive one point.
Performance on the MIS shows little effect from education level. (Someone who has gone to school through 6th grade should be able to perform just as well as someone with a college education.)
Remember that the MIS is a screening tool, not a definitive diagnostic tool. Poor performance on the MIS indicates that there may be a reason to be concerned, but a full physician assessment is necessary to evaluate cognition and eventually diagnose dementia. Keep in mind that there are some causes of memory impairment that can be at least partially reversible with diagnosis and appropriate treatment, such as vitamin B12 deficiency, medication interactions, delirium, and normal pressure hydrocephalus.

Alzheimer"s disease is a brain disorder that gets worse over time. It"s characterized by changes in the brain that lead to deposits of certain proteins. Alzheimer"s disease causes the brain to shrink and brain cells to eventually die. Alzheimer"s disease is the most common cause of dementia — a gradual decline in memory, thinking, behavior and social skills. These changes affect a person"s ability to function.
The early signs of the disease include forgetting recent events or conversations. Over time, it progresses to serious memory problems and loss of the ability to perform everyday tasks.
Memory loss is the key symptom of Alzheimer"s disease. Early signs include difficulty remembering recent events or conversations. But memory gets worse and other symptoms develop as the disease progresses.
Everyone has memory lapses at times, but the memory loss associated with Alzheimer"s disease persists and gets worse. Over time, memory loss affects the ability to function at work or at home.
Alzheimer"s disease causes a decline in the ability to make sensible decisions and judgments in everyday situations. For example, a person may make poor choices in social settings or wear clothes for the wrong type of weather. It may become harder for someone to respond to everyday problems. For example, the person may not know how to handle food burning on the stove or decisions when driving.
Routine activities that require completing steps in order become a struggle. This may include planning and cooking a meal or playing a favorite game. Eventually, people with advanced Alzheimer"s disease forget how to do basic tasks such as dressing and bathing.
Despite major changes to memory and skills, people with Alzheimer"s disease are able to hold on to some skills even as symptoms get worse. Preserved skills may include reading or listening to books, telling stories, sharing memories, singing, listening to music, dancing, drawing, or doing crafts.
A number of conditions can result in memory loss or other dementia symptoms. Some of those conditions can be treated. If you are concerned about your memory or other thinking skills, talk to your health care provider.
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
Scientists believe that for most people, Alzheimer"s disease is caused by a combination of genetic, lifestyle and environmental factors that affect the brain over time. In less than 1% of cases, Alzheimer"s is caused by specific genetic changes that almost guarantee a person will develop the disease. In these cases, the disease usually begins in middle age.
The development of the disease begins years before the first symptoms. The damage most often starts in the region of the brain that controls memory. The loss of neurons spreads in a somewhat predictable pattern to other regions of the brain. By the late stage of the disease, the brain has shrunk significantly.
Plaques. Beta-amyloid is a fragment of a larger protein. When these fragments clump together, they appear to have a toxic effect on neurons and to disrupt communication between brain cells. These clumps form larger deposits called amyloid plaques, which also include other cellular debris.
Increasing age is the greatest known risk factor for Alzheimer"s disease. Alzheimer"s isn"t a part of typical aging. But as you grow older, the chances of developing it increases.
One study found that every year there were four new diagnoses per 1,000 people ages 65 to 74. Among people ages 75 to 84, there were 32 new diagnoses per 1,000 people. For those 85 and older, there were 76 new diagnoses per 1,000 people.
A better understood genetic factor is a form of the apolipoprotein E (APOE) gene. A form of the gene, APOE e4, increases the risk of Alzheimer"s disease. About 25% to 30% of the population carries an APOE e4 allele. But not everyone with this form of the gene develops the disease.
Scientists have found rare changes in three genes that virtually guarantee a person who inherits one of them will develop Alzheimer"s. But these changes account for less than 1% of people with Alzheimer"s disease.
Many people with Down syndrome develop Alzheimer"s disease. This is likely related to having three copies of chromosome 21. Chromosome 21 is the gene involved in the production of the protein that leads to the creation of beta-amyloid. Beta-amyloid fragments can become plaques in the brain. Symptoms tend to appear 10 to 20 years earlier in people with Down syndrome than they do for the general population.
Someone with mild cognitive impairment (MCI) has a decline in memory or other thinking skills that is greater than usual for the person"s age. But the decline doesn"t prevent the person from functioning in social or work environments.
However, people with MCI have a significant risk of developing dementia. When MCI affects mainly memory, the condition is more likely to progress to dementia due to Alzheimer"s disease. A diagnosis of MCI offers people the chance to put a greater focus on healthy lifestyle changes and to come up with strategies to make up for memory loss. They also can schedule regular health care appointments to monitor symptoms.
These factors can all be modified. Therefore, changing lifestyle habits can to some degree alter your risk. For example, regular exercise and a healthy low-fat diet rich in fruits and vegetables are related to a lower risk of Alzheimer"s disease.
Studies have found that socializing and engaging in activities that stimulate the mind throughout life can lower the risk of Alzheimer"s disease. Low education levels — less than a high school education — appear to be a risk factor for Alzheimer"s disease.
Alzheimer"s symptoms such as memory loss, language loss, impaired judgment and other brain changes can make it harder to manage other health conditions. A person with Alzheimer"s disease may not be able to:
This tablet doesn’t require Wi-Fi; it can send and receive data through a 4G LTE connection. In fact, its large 1920×1200 full HD display is perfect for seniors who prefer a larger screen and text. It comes complete with colorful icons and large text to make it easier for seniors experiencing memory or vision loss. If you’re an older adult with dementia, you can use the simplified video chat feature to stay connected with loved ones. With loud speakers and dual speakers, you can easily browse the internet, listen to music, or play popular games like sudoku or other brain games to improve memory.
The GrandPad is user-friendly and great for users who have minimal experience using tablets or cell phones. When I turned on the device, I was able to watch the welcome video, which reviewed all of the important features of the tablet, ranging from photos to contacts. I liked that this tablet lets you create a private circle where a family administrator can be in charge of managing the GrandPad and creating a close circle of family contacts. With the GrandPad, there’s no dialing or typing required; all you have to do is simply touch the screen and click on large fonts and buttons to navigate and connect with loved ones. For instance, when I wanted to make a call, all I had to do was click on the photo of a loved one, and it automatically placed a call.


 Ms.Josey
Ms.Josey 
 Ms.Josey
Ms.Josey